Homebuilt Accidents: The Pilot’s Condition
Flying any aircraft—homebuilt or not—requires the pilot to be alert. The person at the stick has to have their brain firing on all cylinders. But occasionally they don’t.

Image: FAA
By Ron Wanttaja
This story originally appeared in KITPLANES.
Flying any aircraft—homebuilt or not—requires the pilot to be alert. The person at the stick has to have their brain firing on all cylinders. But occasionally they don’t. Sometimes the pilot is flying on the wrong medicine, legal or not. Sometimes the pilot’s body has unknown (or even known) medical conditions that flare up at exactly the wrong time. But how often does it happen?
It’s certainly not just a homebuilt issue. But pilot issues such as substance impairment or medical are already identified in my 1998–2017 homebuilt accident database. It’s a pretty easy task to extract them. Let’s lop off this low-hanging fruit and see where it takes us.
For the purposes of this analysis, let’s use the term “substance impairment” to refer to cases where the NTSB says the pilot’s use of legal or illegal substances may have contributed to the accident. We’ll use “medical incapacitation” for cases where the pilot’s physical health interfered with their ability to control the aircraft.
There were 112 cases of either type in my 20-year homebuilt database—that’s an average of almost six per year, about 3% of all homebuilt accidents.
Substance Impairment
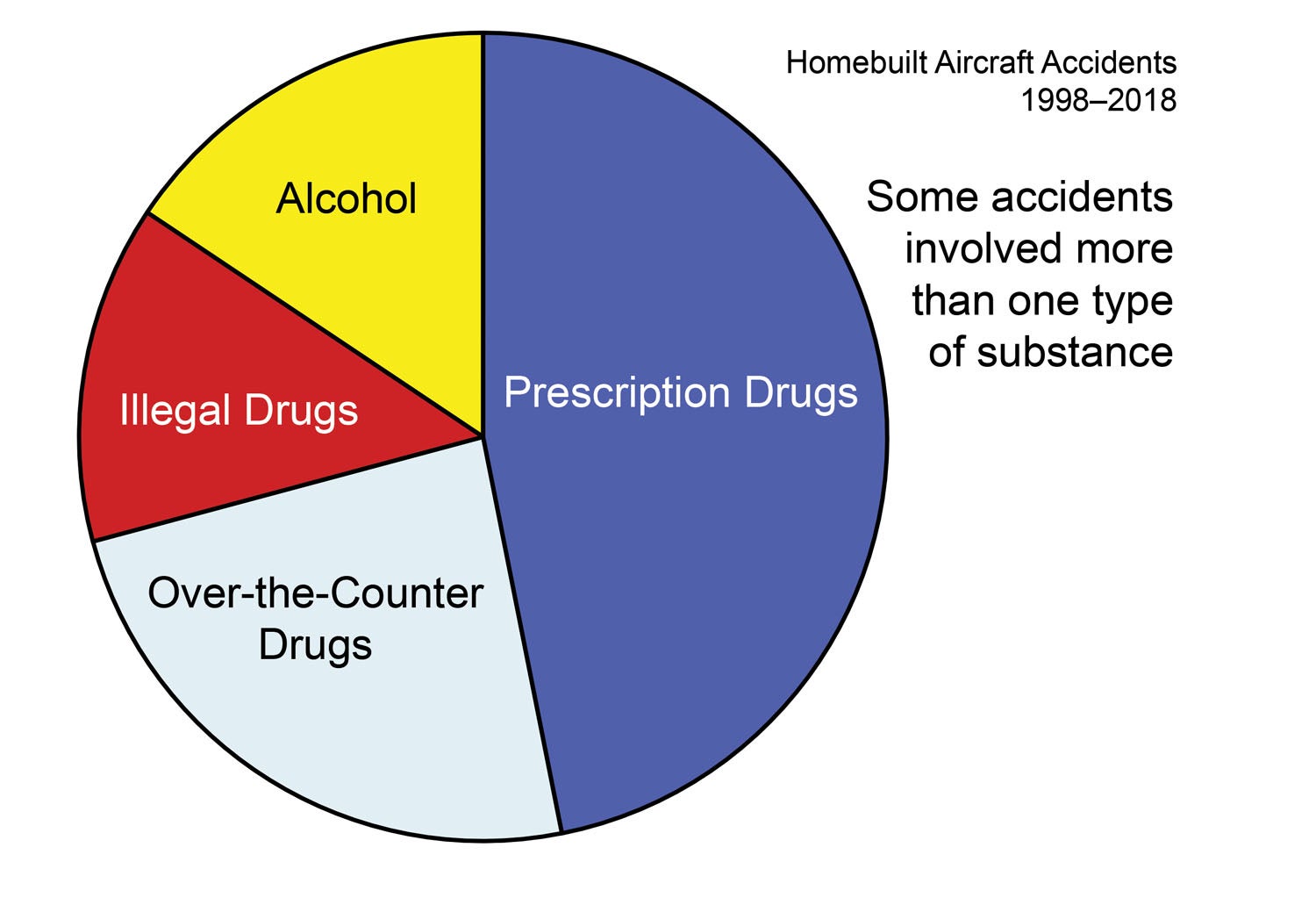
What are the substances in “substance impairment”? Let’s break them into four categories: alcohol, illegal drugs, prescription drugs, and over-the-counter (OTC) drugs.
As Figure 1 shows, the majority of substances involved were legal drugs: prescription and OTC. Almost 75% of the cases included prescription or OTC drugs that have known effects on pilot skills. Alcohol was present in only 15 of 87 substance impairment accidents, illegal drugs in 13. Ten of the accidents noted multiple substance categories.
The most common OTC drugs were antihistamines. If the instructions state not to drive or operate heavy machinery, assume your Kitfox qualifies as “heavy machinery.” Second place were decongestants, usually in combination with the antihistamines.
One accident report (FTW01LA168) contained an interesting bit of insight into the effect of diphenhydramine, a common antihistamine used in OTC products such as Benadryl: “The American College of Physicians-American Society of Internal Medicine conducted a study…on the effects of diphenhydramine on driving performance. Participants had significantly better coherence after taking alcohol or fexofenadine (Allegra) than after taking diphenhydramine…”
In other words, it affects drivers more strongly than alcohol.
The FAA has a guide to OTC medicines.
Of the 13 cases where illegal drugs were detected, one was cocaine, the rest were marijuana. Most of the marijuana cases predate states’ legalization actions. Of course, the drug continues to be illegal under federal law and a bad item to combine with flying on any planet.
The NTSB ruled that the substance was the accident’s probable cause in only four of the 87 cases. In the rest, its presence was noted as a contributor. Typically, the results of the blood tests are noted and the potential effect described, but the degree that it actually affected the outcome is not known.
Medical Incapacitation
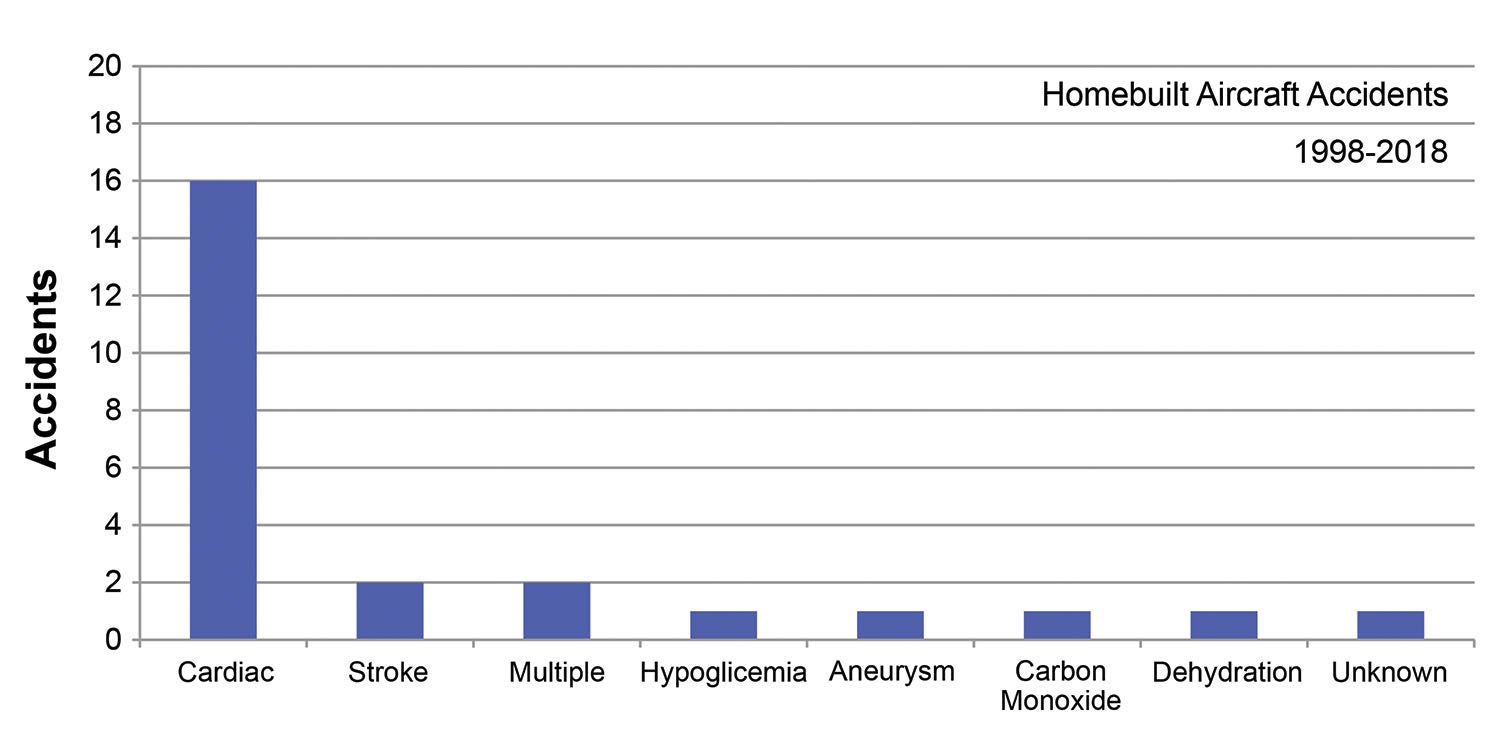
As Figure 2 shows, heart problems predominate in medical incapacitation accidents. Of 25 cases in the homebuilt world in a 20-year span from 1998 through 2018, 16 were attributed to cardiac events. But as author Robert Heinlein said, “In the end, all forms of death can be classed as heart failure.”
A commenter on my recent KITPLANES® article on ADS-B questioned the wisdom of taking legal advice from an engineer (burn!). An engineer offering medical wisdom is an even bigger stretch.

With that said, the autopsies in the NTSB reports in those cases indicate a high probability of the pilots having suffered a cardiac event. But often there isn’t a true smoking gun that a layman like myself can point at and say, “Ah-ha!” But to paraphrase another famous line from science fiction, “Dammit Jim, I’m an engineer, not a doctor!” I’ll bow to medical opinion.
With that, I’ll turn my attention to two cases where I actually have some experience.
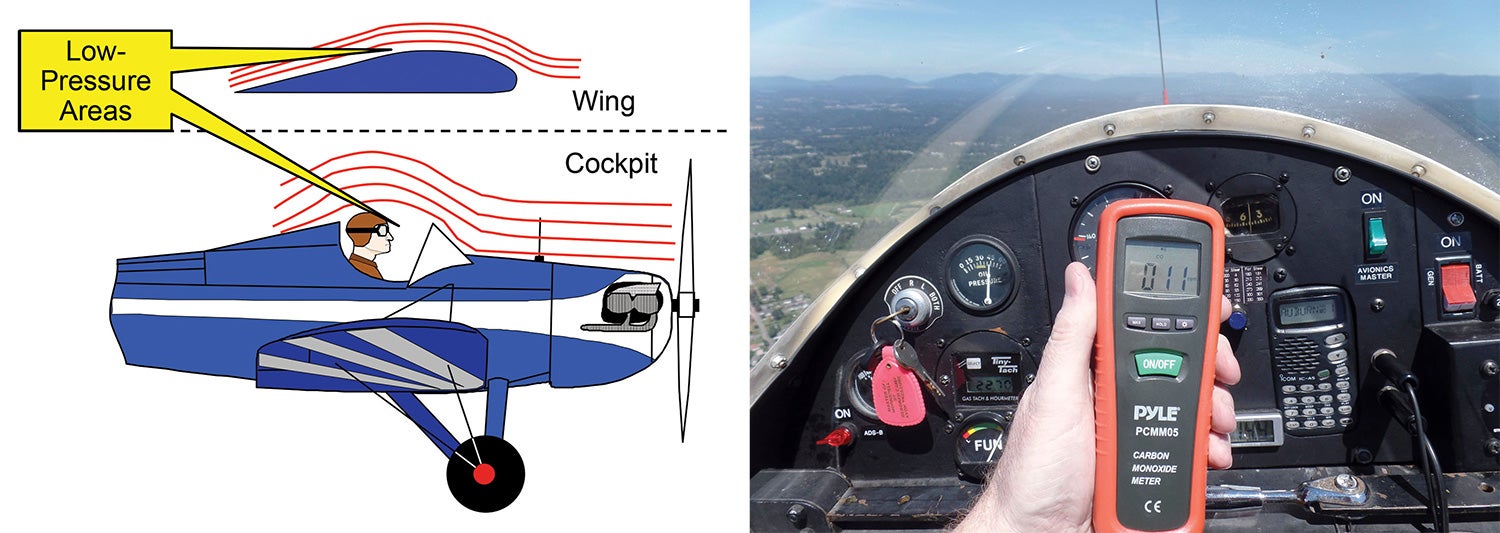
The case of incapacitation due to carbon monoxide (CO) poisoning hit home because I once suffered CO poisoning on a night flight as a passenger in a Mooney. I passed out after landing. There are a lot of ways exhaust gasses can make it into aircraft cockpits, and it can be quite sneaky. I bought a portable CO detector for my airplane, and check it every several months.
And yes, I fly an open-cockpit airplane. Windshields produce a low-pressure area that can draw exhaust fumes into where the pilot is sitting, whether there’s a canopy or not. I have a friend who suffered CO poisoning in a Starduster.
The second case involved probable dehydration. I’ve noticed its effect when flying my Fly Baby on sunny days. Sure, the temperature might be comfortable, but the sun cooks my noggin on hot days on long flights. The dehydration case involved the pilot of an RV-7; the bubble canopy does let the occupants bake a bit. Tuck a water bottle into the cockpit.
Medical Incapacitation and Sport Pilot
Back when the FAA approved Sport Pilot, there was controversy. Pilots of light, simple, slow aircraft would no longer be required to pass periodic medical examinations. Would Light Sport Aircraft fall from the sky, brought down by pilots developing undetected medical conditions?
Twenty-five cases of incapacitation in homebuilt aircraft from 1998 through 2017 aren’t an adequate basis for an assessment—only three involved pilots operating under Sport Pilot. Instead, let’s look at accidents involving all types of aircraft from 1998 through 2017. We’ll search for mention of incapacitation or impairment in their probable causes. Only cases that involved the onset of health issues were included. Cases involving substance use, carbon monoxide, hypoxia and fatigue were eliminated.
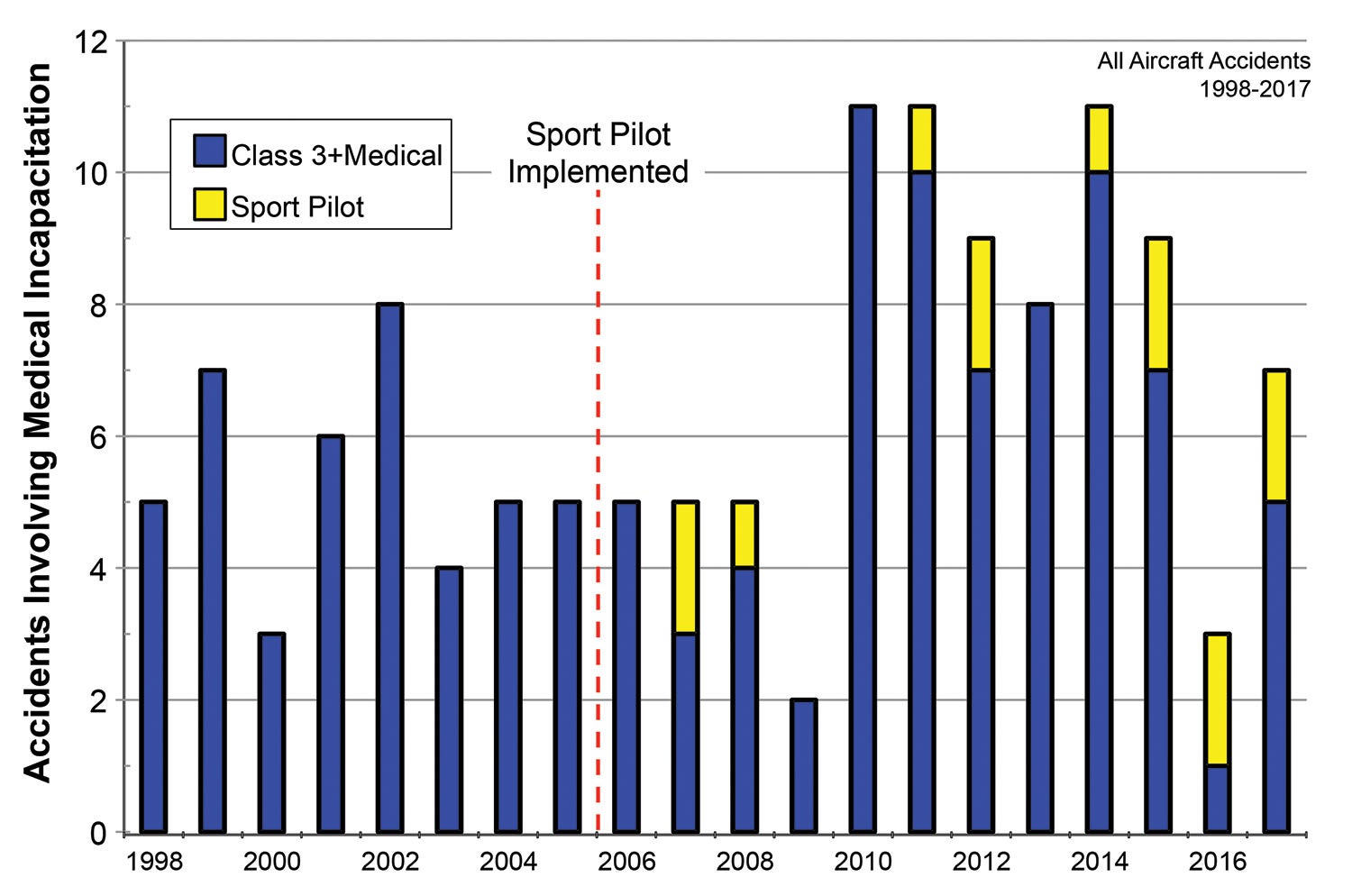
Over the 20-year period examined, 142 cases were found. The results are shown in Figure 3. The dark blue bars show the number of cases per year that occurred to pilots with valid FAA medical certificates (including BasicMed). Yellow bars show how many accidents happened due to medical emergencies suffered by pilots operating under Sport Pilot. The combined height of the bars is the total for that year.
The contribution of Sport Pilot to the statistics is minor. There were 13 cases of pilot incapacitation involving Sport Pilots, about one per year since the program started in 2006. The year 2010 saw the most pilot incapacitation cases; all 11 cases involved pilots with valid FAA medicals. In no year does the combined valid medical and Sport Pilot cases exceed what was witnessed for pilots with valid medicals alone in 2010.

Wrap-Up
The term, “bright-eyed and bushy-tailed” dates from before the Wright brothers, but it does sum up the ideal condition of the pilot of an aircraft. Except for the tail part.
Pilots have to be aware of the effects of over-the-counter medicines, especially antihistamines. We fly Experimental/Amateur-Built aircraft: By definition, all our flying is recreational. If you’ve got a cold or allergies bad enough to need to take over-the-counter nostrums, forego the recreational flying. If your doctor has you on a prescription medicine, be sure to check whether flying under its influence is still allowed.
Not much to be said about those cases involving alcohol or illegal substances. Pilots who imbibe prior to (or during) flight aren’t listening to FAA and medical directives; they aren’t likely to be swayed by me. It will be interesting to see if cases involving marijuana increase as it is legalized in more states. It’s still prohibited as far as the FAA is concerned.
The incapacitation issue is thorny. Traditionally, pilots have adversarial relationships with medical examiners. After all, they can deny us access to the sport we love for reasons we view as esoteric or trivial. Hiding health problems from AMEs has a long history in aviation.
Like all authority figures, though, they aren’t always wrong. About 0.5% of homebuilt accidents were due to pilot incapacitation. Of the 25 cases, 21 were fatal to the pilot. Maybe they could have survived the heart attack/stroke/hypoglycemia, but the planes couldn’t land themselves. The conditions involving physical incapacitation often manifest themselves without the sufferer’s knowledge. That’s where regular physical examinations come in.
Finally, it appears that an average of slightly more than one incapacitation accident per year occurs to a Sport Pilot. Whether this is “acceptable” or not probably depends on one’s view of the program. Those against it will consider a single accident per year as being too many, while those flying under the rule consider it an acceptable risk. It’s likely, though, that without Sport Pilot, many would have continued to fly without FAA medicals. Thirteen Sport Pilots suffered incapacitation from 2006 to 2017—but 10 others met the same fate without valid medical certification.* Not having the Sport Pilot program would not necessarily have prevented 13 accidents; it’s likely some of the pilots affected would have continued without a medical.
We like to say that anyone can fly. For the most part, it’s true—but that “anyone” had better be at the peak of their game. Be wary of your alcohol and drug intake. And Sport Pilot or not, get regular checkups to ensure you’re healthy enough to fly.
*The pilot was flying an aircraft that required at least an FAA Class 3 medical or had failed their medical examination and were thus not legal to fly as a Sport Pilot.





